Renal Trauma
Renal Trauma: Diagnosis, Imaging Evaluation, Grading, and Management
Overview
Renal trauma represents approximately 10% of all abdominal injuries and is most often secondary to blunt mechanisms such as motor vehicle collisions, falls, or sports injuries. Penetrating injuries (gunshot, stab wounds) account for a smaller but more severe subset. Early and accurate diagnosis, particularly through imaging, is critical to guide management, preserve renal function, and prevent unnecessary nephrectomy.
Initial Clinical Assessment
Key Indicators
• Hemodynamic status dictates urgency. Unstable patients with expanding retroperitoneal hematoma generally require surgical exploration.
• Hematuria: Gross hematuria strongly suggests renal injury, but absence does not exclude significant trauma, particularly vascular pedicle avulsion or thrombosis.
• Mechanism: High-velocity deceleration or flank impact is a red flag.
• Physical findings: Flank ecchymosis, flank mass, rib or transverse process fractures, or palpable tenderness should prompt imaging.
Laboratory Evaluation
Serum creatinine and hematocrit for baseline renal function and blood loss. Urinalysis to detect hematuria or infection. Serial monitoring guides progression or resolution.
Imaging Evaluation
Imaging Indications
• Gross hematuria, or microscopic hematuria with hypotension (SBP <90 mm Hg)
• High-energy mechanism with flank ecchymosis or associated injuries
• Penetrating trauma to the flank or upper abdomen
• Pediatric patients with any degree of hematuria following blunt trauma
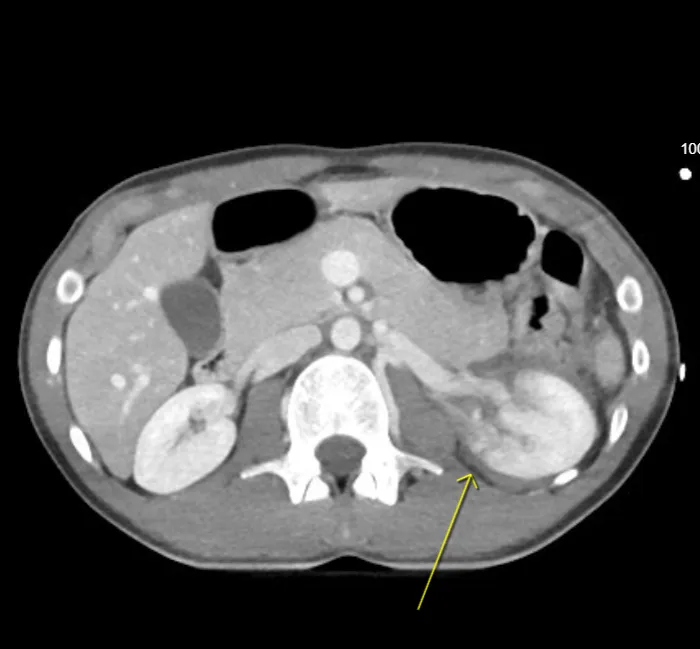
Preferred Modality: Contrast-Enhanced CT Abdomen and Pelvis
CT is the gold standard for both diagnosis and grading of renal injury. It defines parenchymal lacerations, vascular involvement, collecting-system disruption, and urinary extravasation with high accuracy.
CT Protocol Optimization
1. Non-contrast phase – Detects pre-existing stones, acute hemorrhage, or contrast extravasation on subsequent phases.
2. Corticomedullary phase (25–40 s) – Demonstrates active arterial bleeding or vascular disruption.
3. Nephrographic phase (80–100 s) – Characterizes parenchymal lacerations, infarcts, and hematomas.
4. Excretory/delayed phase (5–10 min) – Evaluates collecting-system integrity and urinary extravasation.
Optional: Split-bolus or dual-energy CT can reduce total contrast dose while preserving phase information.

Radiologist’s and Clinicians Role
1. Clinicians provide clinical history regarding trauma class, blood in urine, bruising, focal pain.
2. Radiologist-Injury Detection and Characterization
Radiologists play a central role in triaging renal trauma. Beyond confirming injury, the report should include:
• Location (upper/mid/lower pole; anterior/posterior)
• Extent and depth of laceration
• Collecting-system involvement (extravasation pattern)
• Vascular injury (pseudoaneurysm, active extravasation, thrombosis, dissection, pedicle avulsion)
• Associated findings: perirenal hematoma, urinoma, retroperitoneal extension, adjacent organ injury
3. Recognizing Imaging Patterns
• Contusions: Ill-defined hypoattenuation without cortical disruption.
• Lacerations: Linear or branching low-attenuation defects extending from cortex inward.
• Segmental infarction: Wedge-shaped non-enhancing region due to vascular occlusion.
• Collecting-system disruption: Delayed phase contrast extravasation.
• Vascular pedicle injury: Abrupt arterial cutoff or non-enhancement.
• Active hemorrhage: High-density jet of contrast on dynamic phases.
4. Pitfalls and Mimics
• Renal clefts may mimic lacerations—smooth margins, no hematoma.
• Beam-hardening artifact can simulate extravasation—verify on delayed phase.
• Transient ischemia or vasospasm can mimic infarct—resolves on follow-up.
5. Radiology Reporting
1. Mechanism of injury and indication
2. Renal findings (laceration size, pole, collecting-system involvement)
3. Perirenal/retroperitoneal findings (hematoma, urinoma, abscess)
4. Associated injuries (adrenal, liver, spleen, bone)
5. AAST grade and recommendation (with rationale)
6. Post-Treatment and Follow-Up Imaging
• Follow-up CT (48–72 h) for Grade III–V or clinical concern.
• Ultrasound for hematoma or urinoma resolution.
• Monitor for complications: pseudoaneurysm, AV fistula, urinoma, abscess.
• Long-term follow-up: monitor blood pressure and renal function.
Management Overview
Non-operative (Preferred for Stable Patients)
Observation, bed rest, serial hematocrits, fluid management, antibiotics if needed, and interventional radiology for embolization if bleeding persists.
Operative
Indicated for instability or vascular pedicle avulsion. Aim for renal preservation whenever possible.
Key Takeaways
• CT with excretory phase is essential for complete evaluation.
• Radiologists should include grade, vascular detail, and management relevance.
• Over 80% of renal injuries are managed non-operatively.
• Structured, concise reports improve multidisciplinary outcomes.

